
65 year old male with asymmetric upper extremity blood pressure readings and left arm fatigue with activity.
-

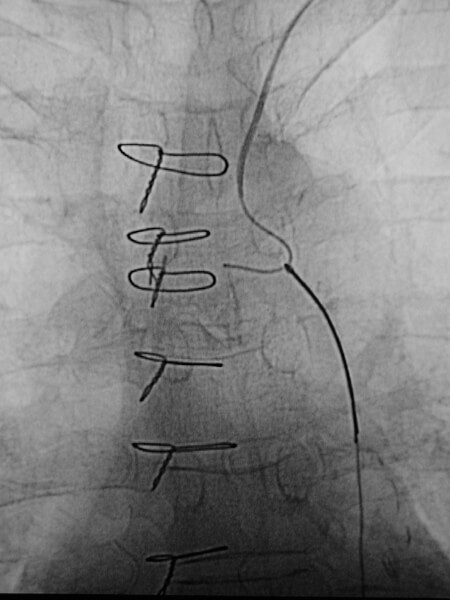
Early image from a thoracic aortogram demonstrating occlusion of the left subclavian artery. -

Lagte image from a thoracic aortogram demonstrating reconstitution of the left subclavian via retrograde flow in the left vertebral artery. -
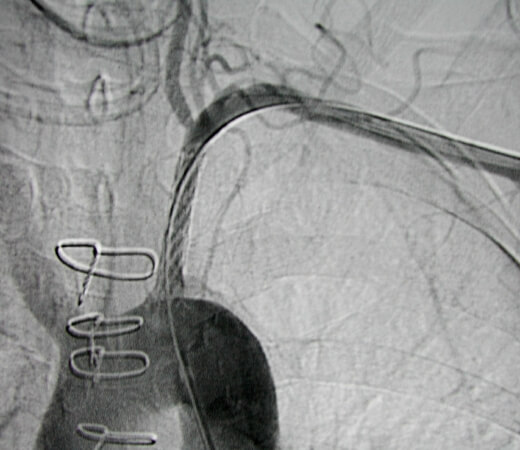
Single image showing the upper extremity catheter access enabled guidewire passage across the occlusion. A snare was placed from common femoral artery access and used to capture the wire, enabling "through and through" access across the occlusion. -
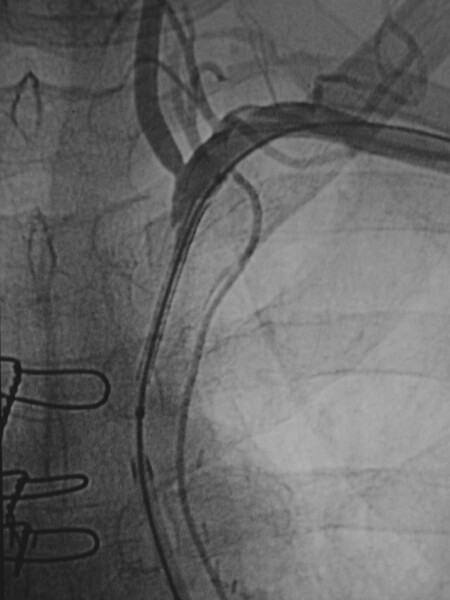
Once access was achieved across the occlusion, a long sheath was placed from the common femoral artery across the occlusion. -
Final image after placement of a balloon expandable stent demonstrating restored patency of the proximal left subclavian artery.
Comment: Given the left subclavian artery occlusion at the origin with almost none of the occluded vessel evident on the thoracic aortogram, it was best to gain upper extremity arterial access to facilitate the attempt at crossing the occlusion. Once we were able to cross the occlusion, we didn’t want to place the sheath needed for stent placement. Therefore, we used a snare to capture the guidewire and ultimately placed a balloon-expandable stent across the occlusion from a common femoral artery approach.